Strengthening Ethiopia’s Response to Polio: AFENET Supports National Co-administration Campaign in Afar Region
-
by
AFENET


Ethiopia has intensified its efforts to interrupt poliovirus transmission following continued outbreaks of circulating vaccine-derived polioviruses (cVDPVs) especially type 2 (cVDPV2) and the recent detection of type 1 isolates (cVDPV1) through environmental surveillance. In response, the country launched a nationwide supplementary immunization campaign in October 2025 using a co-administration strategy with both bivalent oral polio vaccine (bOPV) and novel oral polio vaccine type 2 (nOPV2). This innovative strategy aims to rapidly boost population immunity and halt ongoing transmission.
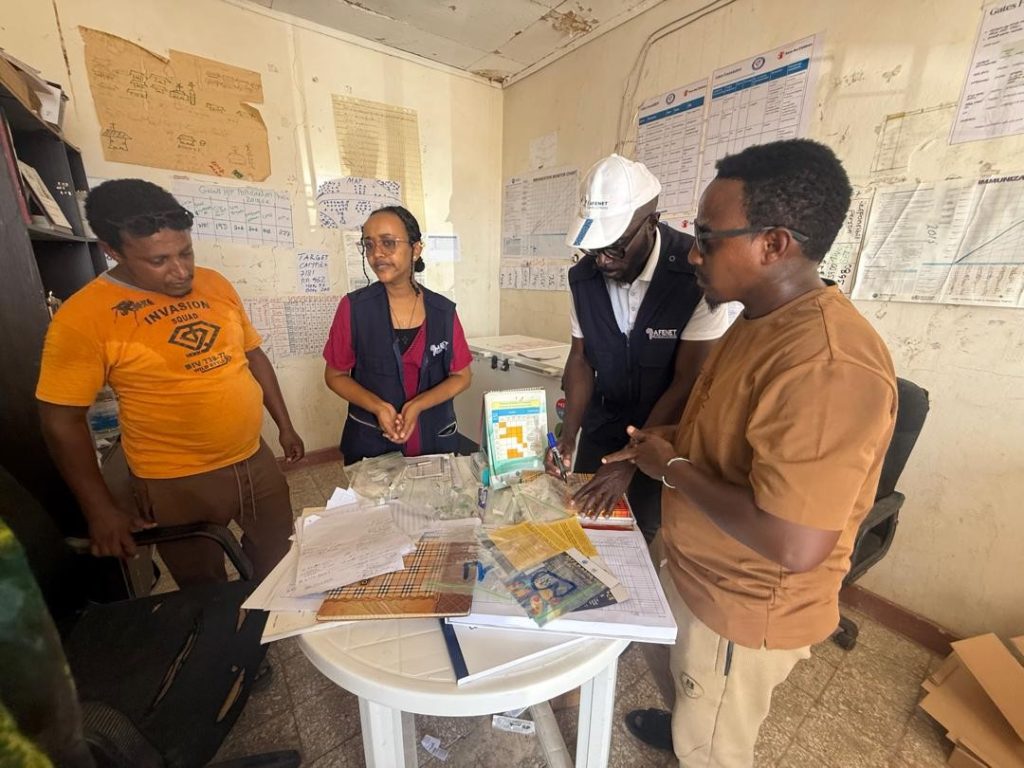
From 7–15 October 2025, AFENET deployed a technical mission to Ethiopia with a special focus on the high-risk Afar Region, providing critical support to planning, implementation, supervision, and real-time mentoring throughout the campaign.
Polio Risk Landscape in Ethiopia
By 2025, Ethiopia had recorded a cumulative 40 cVDPV2 cases, with Oromia Region accounting for 30 cases. The Afar Region where AFENET’s field supervision was centered remains particularly vulnerable due to:
- High levels of population mobility
- Frequent cross-border movements
- Refugee settlements.
- Risk of importation from neighboring countries, including detection of cVDPV1 in Djibouti, which borders Afar
To address these risks, the Ministry of Health and partners organized a nationwide co-administration campaign from 10–13 October 2025, with two additional days allocated for low-performing areas. The campaign targeted 22 zones across seven regions, aiming to reach 7,923,294 children, including:
- Children under five years across 16 zones
- Children under ten years across six zones
The campaign benefited from strong collaboration among the Ministry of Health, Ethiopian Public Health Institute (EPHI), WHO, UNICEF, Gavi, CDC, AFENET, and TFGH working together to improve campaign quality, strengthen surveillance, and ensure no child was left behind.
Purpose of the AFENET Mission
AFENET’s mission focused on delivering targeted technical support to EPHI and the Afar Regional Health Bureau (RHB). Key priorities included:
- Assessing preparedness and coordination at regional, woreda, health facility, and community levels
- Providing real-time mentorship to field teams on:
- Vaccine handling and safe administration
- Cold chain and logistics management
- Data recording, reporting, and accountability
- Acute flaccid paralysis (AFP) and polio surveillance
- Community engagement and social mobilization
- Identifying operational gaps and providing immediate corrective recommendations
- Supporting partners in reviewing the co-administration evaluation protocol and planning for its implementation
This hands-on approach aimed to improve adherence to national and global standards and enhance the overall quality and impact of future immunization rounds.
Mission Activities and Early Coordination
Tuesday, 7 October 2025 – Arrival and Initial Briefing
The AFENET team arrived in Ethiopia on the afternoon of 7 October and immediately participated in a coordination meeting at the AFENET office with Dr. Tatek Bogale, AFENET Horn of Africa Regional Technical Coordinator.
Discussions focused on:
- Reviewing AFENET’s planned support for the polio campaign in Afar
- Outlining coordination with national and subnational stakeholders
- Preparing for discussions with EPHI, the Ministry of Health, and CDC Ethiopia
- Reviewing expectations for the CDC-requested evaluation of the co-administration campaign
Arrangements were made to consult with CDC colleagues to refine evaluation methodologies and ensure strong monitoring and accountability mechanisms.
Wednesday, 8 October 2025 – Engagement with EPHI and CDC Ethiopia
On 8 October, AFENET and CDC Ethiopia held a series of technical meetings at EPHI. AFENET, represented by Dr. Tatek Bogale, joined the CDC Immunization Team including Dr. David Schnabel and Dr. Kumie Shiferaw to align partner roles for the campaign.
Key areas discussed included:
- Preparedness for the national bOPV–nOPV2 co-administration effort
- Harmonizing technical support, supervision, and monitoring roles
- Reviewing the evaluation protocol led by Edward Dagoe, who was scheduled to travel to Ethiopia for further technical support
Follow-up actions included:
- Scheduling a detailed session with Dr. Dagoe to clarify methodology, budget, and logistical considerations
- Ensuring continuous engagement with Mikias Alayu, VPDs Surveillance and Response Lead at EPHI, for leadership oversight and sustained support
These strategic engagements strengthened partner alignment and enhanced readiness for effective campaign implementation in Afar and nationwide.
Looking Ahead
The initial days of the mission were crucial in setting a strong foundation for execution, monitoring, and evaluation of Ethiopia’s co-administration campaign. Through collaboration with EPHI, Afar RHB, CDC, and other partners, AFENET continues to contribute significantly to:
- Strengthening field supervision and real-time capacity building
- Enhancing data quality, reporting, and accountability
- Supporting community engagement and risk communication efforts
- Advancing evidence-based evaluation of innovative immunization strategies
These contributions are vital for protecting children in high-risk regions like Afar and sustaining progress toward a polio-free Ethiopia and Horn of Africa.
Thursday, 9 October 2025 – arrival in Afar region and precampaign activities
- Arrival in Semera and meeting with AFENET Polio Consultant:
- On arrival in Semera from Addis Ababa, met with Ms. Helen Atkilt Siyoum, AFENET consultant, who provided updates on campaign preparations in the Afar Region. Overall readiness was good — health worker trainings were underway, vaccines and cold chain materials had been delivered, and LQAS training was being conducted by WHO in Semera on the same day.
- Identified Gaps: Key issues highlighted included a late start of social mobilization activities and anticipated delays in fund transfers for field team allowances.
- As far as Helen’s routine field work is concerned, field activities are proceeding well in her region of deployment, Gambella, with no major challenges reported.
- Pre-Campaign Supervision in Asaita Woreda: Travelled to Asaita Woreda for supervision prior to campaign launch. Visited the woreda health office cold chain and met with campaign supervisors, including the Public Health Emergency Management (PHEM) Officer, EPI Officer, Social Mobilizer, and Vaccine Accountability Manager (VAM) to assess readiness.
- Cold chain and logistics assessment: Evaluated the cold chain system and verified availability of essential logistics and data tools such as tally sheets and VAM forms. Conducted on-site mentorship on vaccine retrieval, emphasizing correct labelling, use of ziplock and plastic bags differentiated by vaccine type, and reviewed availability of finger markers and chalk for household marking during the campaign.
- Microplan and readiness review: Reviewed campaign microplans, confirming 16 vaccination teams, 4 team supervisors, vaccine stock levels, and the target population for the woreda. Assessed social mobilization activities, vaccine vial retrieval plans, and the campaign readiness dashboard.
- Health Worker Training Visit: Supervised a training site for health workers, one of the final sessions before campaign start. The training had been successfully conducted by trainers, with vaccination teams ready to resume the campaign the following day. It was also noted that an advocacy meeting with religious leaders had been conducted to support community engagement in the Woreda.
- Asaita woreda has one health center and 13 health posts (8 functional), including six hard-to-reach sites accessible only by camels, which were used to transport vaccines and logistics. A total of 192 vaccine vials (50 doses per vial; wastage factor 1.18) had been received, which was determined to be adequate for the woreda’s target population.
- Challenges and Follow-Up Actions: Identified challenges included delays in social mobilization and limited transportation funds. These issues were promptly communicated to the Regional Health Bureau (RHB) campaign coordinator, who committed to follow-up, and provided pre-recorded audio messages for megaphone use by social mobilization teams.
- Regional Review Meeting: Later in the day, we met with the Afar RHB team at the Public Health Emergency Operations Center (PHEOC) in Semera. Discussions with the PHEM Director and Data Manager focused on regional microplans, logistics status, campaign data management, and plans for last-mile vaccine distribution and vial retrieval.
Friday, 10 October 2025 – Campaign Launch and Day 1 of campaign implementation
- Campaign Launch: The polio campaign officially launched in Logiya town, attended by Afar Regional Health Bureau (RHB) leadership, Afar Public Health Institute (AfPHI), partners, health workers, religious leaders, community members, and the media. The event marked the beginning of the nOPV2 and bOPV co-administration campaign in the region.
- Supervision at Semera Health Center: Conducted an on-site supervisory visit to Semera Health Center, reviewing the campaign microplan, cold chain functionality, and data tools including tally sheets and vaccine accountability forms. Provided mentorship on the correct use of ziplock bags for proper segregation of nOPV2 and bOPV vials, accurate labeling of usable and used vials, as well as the use of 5 kg bag for nOPV2 vial retrieval.
- Vaccination Team Supervision: Proceeded from the health facility to the field to supervise vaccination teams. For the first team supervised in Semera town, observations revealed that teams were equipped with bOPV and nOPV2 vials, but lacked foam pads and proper labeling in vaccine carriers. Gaps were also noted in movement plans and area maps. On-site mentoring was provided on vaccine separation and labeling (using “N” for nOPV2 and “B” for bOPV), and reminders were given regarding AEFI/AFP surveillance. Social mobilizers were advised to move ahead of vaccination teams to ensure community awareness and participation.
- Supervision in Derek Wedeb Village, Semera town: Conducted a second supervisory visit in Derek Wedeb village, observing and supporting the vaccination process. Reviewed cold chain maintenance, data tool usage, and completed the ODK supervisor checklist. The team was correctly administering both bOPV and nOPV2, though they also lacked foam pads in carriers. By 5:00 p.m., only 60 of the expected 200 children had been vaccinated, mainly due to a late start and a pause for Friday prayers, which slowed team progress.
- Operational Observations: Identified that late starts and prayer breaks contributed to slower daily coverage and reduced output for some teams.
- Regional Coordination Call: Participated in the first daily regional coordination call at 7:40 p.m., where the main issue raised was transportation constraints affecting team movement and vaccine distribution. All Woredas had otherwise started the campaign. Strategies were laid out to proceed successfully with day 2 of the campaign, including teams resuming vaccination early, and addressing specific comments
Saturday, 11 October 2025 – Day 2 of campaign implementation
- Supervision in Dicheto, Elidar Woreda: Conducted supervisory visits in Dicheto kebele, including border areas adjacent to Djibouti, to assess campaign progress and field implementation.
- Campaign Performance: The woreda had achieved 98% of its target for Day 1, demonstrating strong initial performance.
- Identified Gaps: Several issues were observed, including a shortage of Vaccine Accountability Management (VAM) forms, use of woreda-level tools at health facility level, missing batch numbers, incomplete vial usage and return records, incorrect house and finger marking, and limited community awareness regarding AFP and AEFI surveillance.
- Border Site Challenges: It was noted that there was no dedicated vaccination team at the Galafi border crossing, and social mobilization efforts were weak in the area. These gaps were reported during the evening coordination call for immediate corrective action.
- Field Supervision: Supervised two vaccination teams in the field (one in Dicheto and one in Galafi) and conducted inside household monitoring in 10 households. Corrected observed errors, particularly in house marking practices.
- Movement Plans: Reviewed daily movement plans, which were found to be in use and properly followed by the teams.
- AFP Surveillance: Teams were not conducting AFP surveillance during their activities and were reminded of the importance of active case detection and reporting.
- Vaccine Handling: Observed that teams were mixing nOPV2 and bOPV vials; mentorship was provided on proper vial separation and safe handling procedures.
- Cold Chain Review: Assessed vaccine carrier use and cold chain maintenance, providing guidance on maintaining optimal temperatures throughout the day.
- Vaccination Observation: Observed and supported teams conducting the vaccination of children, ensuring adherence to correct procedures and documentation.
- Inside household monitoring Observation: Visited 10 households with children under five in Dicheto Kebele and observed that finger marking was done incorrectly (on the right little finger). Delivery of key messages was also found to be inadequate. Additionally, 6 missed children were identified—2 were not vaccinated at all, and 4 were vaccinated but not finger marked.
- Cross-Border Coordination: Visited the international border area with Djibouti and provided mentorship to supervisors on establishing a dedicated vaccination post at the crossing point, given the high population mobility and risk of cross-border transmission.
Sunday, 12 October 2025 – Day 3 of campaign implementation
- Conducted campaign supervision in Afambo Woreda. This Woreda had achieved 87% coverage on day 1, and 91% coverage by day 2 of the campaign.
- During vaccination team supervision, teams were observed correctly administering both campaign vaccines, and strong vaccine accountability monitoring was also observed. Challenges faced included marking of temporary shelters, transport gaps, phone network interruptions requiring physical delivery of campaign results at the Woreda health office, and late team deployment.
- Conducted inside-household monitoring for sampled houses in Wedimale village, and used ODK during the supervision. Vaccination teams had reached all households visited, and children were vaccinated. Caregivers reported awareness of the campaign in all households. Teams were inconsistently sensitizing households on AFP cases as well as AEFIs.
- There were some errors observed with finger marking on the wrong hand, as well as some house marking errors. Feedback on these findings was given to the Woreda supervisor for corrective action with the vaccination teams
- Proceeded to Aysaita refugee camp, where we met with the Refugee and Returnee service(RRS) camp manager, as well as the camp EPI supervisor, the Public Health Emergency Management (PHEM) officer as well as a Field Coordinator. The camp had a campaign target population of 1,389 children under 5 years. The camp had 5 vaccination teams assigned, and 1 team supervisor.
- Proceeded to the health center located within the camp, where we reviewed the status of the cold chain, availability of logistics, as well as data tools the previous day’s vaccination. The main challenges mentioned included difficulty marking some camp shelters (made of tarpaulin), and permanent markers had been used to mark such dwellings. Otherwise, all logistics were mentioned to be in place and the exercise was progressing well and on track to achieve the campaign target.
- At the refugee site, in house monitoring conducted showed evidence of high-quality implementation with all children in the sampled houses vaccinated , correct finger and house marking, caregiver awareness of the campaign, and sensitization having been conducted on AFP case detection and reporting, as well as sensitization on AEFIs.
Monday, 13 October 2025 – Day 4 of campaign implementation
- Supervision was conducted in Mille Woreda, where we met with the Woreda EPI Focal Person who was also the VAM for the campaign. We also met with the Woreda Coordinator and PHEM Focal Point
- 28 teams had been deployed. It was reported that six teams lacked transport for the day. We immediately informed the Regional Coordinator, who took action to provide transport support
- We traveled to community level, where team supervision was conducted. The team supervised mentioned having a target of 1,330 children for the 4 days of the campaign. By the third day of the campaign (day before this supervision), they had vaccinated 1,050/1330 and were on track to meet the target
- We proceeded to Adis Ketema village in Adaytu town, where inside-house monitoring was conducted. All sampled houses had eligible children vaccinated. Most of the sampled houses had correct finger and house marking. Gaps observed in some households included incorrect finger marking, and caregivers not asked or sensitized about AFP cases
Tuesday, 14 October 2025
Traveled back to Addis Ababa from Afar region. Conducted debrief meetings and provided updates, including with AFENET RTC Dr. Tatek, CDC Ethiopia colleagues and EPHI, providing updates on the field travel to Afar region. It was also agreed to schedule a follow up conference call with Dr. Edward Dagoe to discuss the evaluation of the coadministration, with the meeting to be held the following week on Tuesday 21st October 2025.
Wednesday, 15 October 2025
Traveled back to Uganda at the end of the mission
- SWOT analysis – coadministration campaign in Afar region
Strengths:
- All Woredas started campaign as scheduled, with teams deployed to the community from day 1
- Campaign launch was successful with key players from national and subnational level present. Key partners supported the launch ceremony, and community members and media were on site to raise awareness
- Daily virtual review meetings were held at regional and national level to track performance and problem solve during the campaign
Weaknesses:
- Errors observed in finger and house marking in some communities
- Incorrect vaccine vial retrieval practices, such as mixing bopv and nopv2 vials in same ziplock
- Lack of foam pads for vaccine carriers in some teams
- Inadequate transport for vaccination teams seen in some Woredas
Opportunities
- Highly motivated staff observed in the field, at Woreda, facility and kebele level
- Presence of dedicated immunization partners/ stakeholders supporting the campaign implementation
- Strong support from local religious leaders during campaign
Threats:
- Hard to reach communities, without road access
- Security situation in some Woredas
- Very high temperatures – this is the hottest region in the country, requiring teams to adequately prepare for the weather conditions
General observations:
Below are some general observations made from the field supervision during the campaign:
- High quality training of vaccination teams is required to ensure a high-quality campaign. This helps minimize errors such as incorrect finger and house marking, giving vaccine to overage children, and poor vaccine accountability practices.
- High quality microplanning is key to adequately plan for transportation of teams. Coadministration requires careful planning to ensure adequate logistics are available, since two antigens are being given at the same time to each child
- Careful cold chain management is required, including vaccine storage at Woreda and health facility level
- Careful administration of vaccine doses by vaccination teams is required to avoid errors in mixing vials and providing doses of the same vaccine twice
- Meticulous management of nOPV2 vaccine vial retrieval as part of vaccine accountability is important, including labeling disposal bags correctly and avoiding mixing empty vaccine vials
5. Recommendations
Below are some proposed recommendations for consideration, for improvement of the next planned campaign, with responsible persons included:
- Strengthen training quality with emphasis on differentiating and handling nOPV2 and bOPV, correct house and finger marking, and AEFI/AFP surveillance integration (RHB campaign coordination team)
- Enhance preparedness validation at least three days before campaigns, with at least 70% site verification (RHB campaign coordination team).
- Ensure timely and efficient social mobilization including in hard-to-reach kebeles and border areas (RHB campaign coordination team).
- Ensure logistical readiness (foam pads, labeling, transport) before campaign start (RHB campaign coordination team).
- Ensure to plan for deployment of vaccination teams at cross-border points.
- Improve data quality and accountability through correct tallying for nOPV2 and bOPV and daily review (Vaccination teams/ campaign supervisors).
- Improve data quality and accountability through correct tallying for nOPV2 and bOPV and daily review (Vaccination teams/ campaign supervisors).
- Ensure correct finger marking and house marking throughout the campaign (campaign supervisors/ vaccination teams)
- Ensure timely retrieval of nOPV2 vials from health facilities to woreda level as per SOP (vaccine accountability managers, campaign supervisors).
6. Conclusion
The polio co-administration campaign in Afar region was successfully launched and implemented, and is on track to achieve good coverage despite some operational challenges and gaps observed. Real-time supportive supervision was conducted and identified and addressed several gaps in cold chain, social mobilization, and field implementation. Strengthened preparedness, training, and logistics—particularly at the last mile—will be essential to sustain quality in future campaigns and to accelerate progress toward stopping transmission.
According to the LQAS results, out of the 13 woredas where the quality survey was conducted, Semera-Logiya town did not meet the minimum LQAS passing criteria, resulting in an overall LQAS performance of 92% for the Afar region. The full campaign administrative coverage results as well as LQAs results will also be shared once availed.